Enlarged Prostate Treatment
Prostatic enlargement is one of the most common problems encountered in men. Around 50% of men in their 50s will have a prostate Enlargement. Half of those require medical treatment. If medicine fails then surgery is the solution.
However, men would be keen to avoid the most common side effects of prostate surgery. These are Mainly dry orgasm and urinary incontinence. Of course, men would be very keen to go back to their normal activities as soon as possible.
What are the side effects of prostate surgery?
There are several types of surgery for prostate enlargement. All have side effects including hospital stay and urinary catheterization, and the above-mentioned side effects.
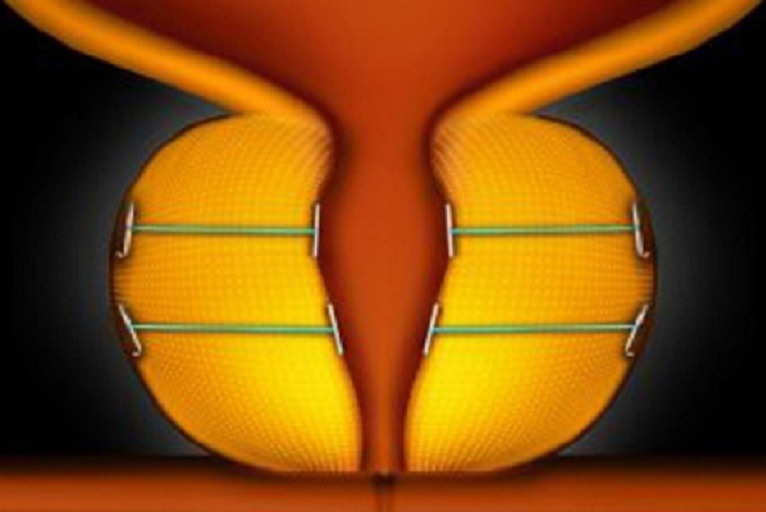
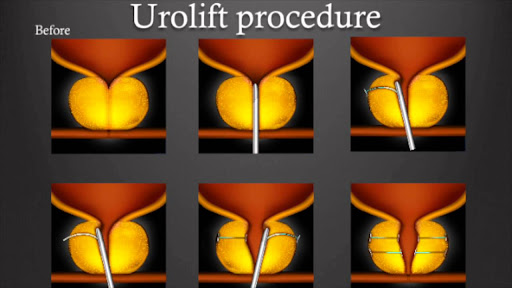
What Is UroLift?
A few years back a new method has emerged. The concept of which included simply pinning the prostate lobes to the side, hence, opening the occlusion created by the prostate Enlargement. This is called prostatic urethral lift, or UroLift.
What are the Benefits of UroLift?
The whole process would take up to 15 minutes. The patient is hardly in need of a urinary catheter afterward. Most would go home on the same day. They would return to their daily activities almost immediately.
However, When first introduced, the UroLift Procedure was largely rejected, because of a lack of knowledge for the long-term effects.
Since then, several trials were carried out and the results were outstanding. The procedure proved its efficacy, safety, and tolerability.
Patient satisfaction was phenomenal. The objective results of the operation including the IPSS score and the flow rate were significant.
UroLift procedure has proven to be even safer for men who are high-risk surgical candidates.
This procedure is simply revolutionary. Intermediate-term results are very encouraging. Long-term effects are still awaited
For Enlarged Prostate Treatment and more information, book an Appointment with Dr. Ali Thwaini on +971 50 435 4853.