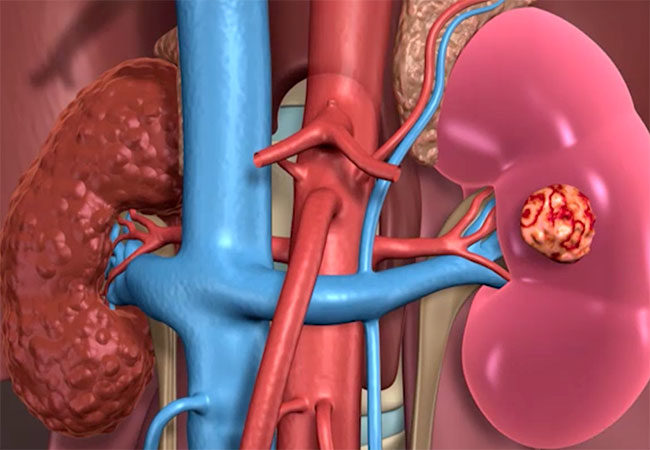
Nephron sparing surgery
Nephron sparing surgery has gained wide acceptance in the past decade or so. After being considered mainly for absolute and some relative indications ( single anatomical or functioning kidney or bilateral renal disease that renders the patient with long-term effects from chronic kidney disease), partial nephrectomy has now topped up the radical nephrectomy in many situations.
Nowadays the most common indication for partial nephrectomy is an elective one ( in the presence of a normal contralateral kidney and a normal overall kidney function.
What are the complications of nephrectomy?
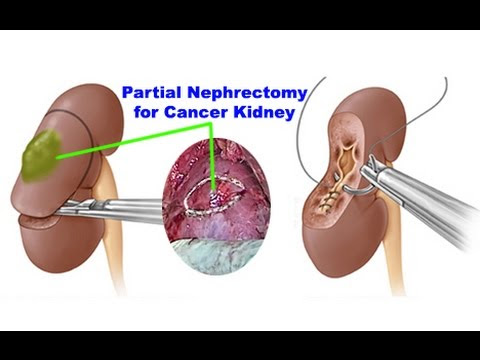
However, there are risks associated with this procedure. Being a very vascular structure, cutting through kidney tissue would inevitably result in bleeding that could be excessive at times. To minimize it, the blood supply is cut during excising the tumour, which should not take more than 30 minutes ( some say 25 min), longer ischemia would result in damage to the remaining kidney tissue.
The other complication is a urine leak. This mainly occurs with complex kidney tumours that are too close to the renal collecting system. This would be at risk of being breached during the time-limited resection and despite an operative repair, still, urine leak might still happen, which would potentially take a longer time to heal and potentially need other procedures. Thirdly, cancer control; tumours should be removed with a clear margin. This traditionally was “estimated” to be 1 cm. Evidently, these large clear margins are not indicated, and wasteful of normal precious kidney tissue. This has now decreased to as little as 1mm.
On the other hand, as much as 20-30% of small renal masses could have a benign nature to them, and active surveillance is now becoming a strong contender to partial nephrectomy, especially in relatively older people who aren’t or are unwilling to go for major surgery. One should not be deceived by the word “partial” here! In this context, partial means major.
Lastly, the dark horse in the race of kidney cancer treatment is the minimally invasive ablative treatment for small renal masses (radiofrequency ablation, cryoablation, microwave).
In summary
Partial nephrectomy is now becoming the gold standard for treating organ confined kidney cancers, when it is technically feasible, and safe to do so.
Having performed over 200 of these procedures, and having harvested the success in most and endured failure of some, along with my patients, I conclude
When offering any kind of treatment, one has to think not only of the organ being treated but health and the quality of life of the human bearing this organ Do No Harm